Observed gap
What we have seen lacking in hospitals outside the default EHR markets
Stratir field work across Latin America, Africa, and South Asia surfaces the same failure mode: clinical teams possess medical expertise, but the hospital lacks a shared operational picture. Beds, referrals, protocols, supplies, and notes live in separate mental models. Directors receive lagging aggregates. Wards improvise with messaging apps and paper fallbacks.
MedicOS research asks how a command surface can close those loops without assuming OECD infrastructure: always-on LAN, dedicated workstations, integrated ADT, and supply APIs that already exist.
Digital maturity versus operational friction across observed regions
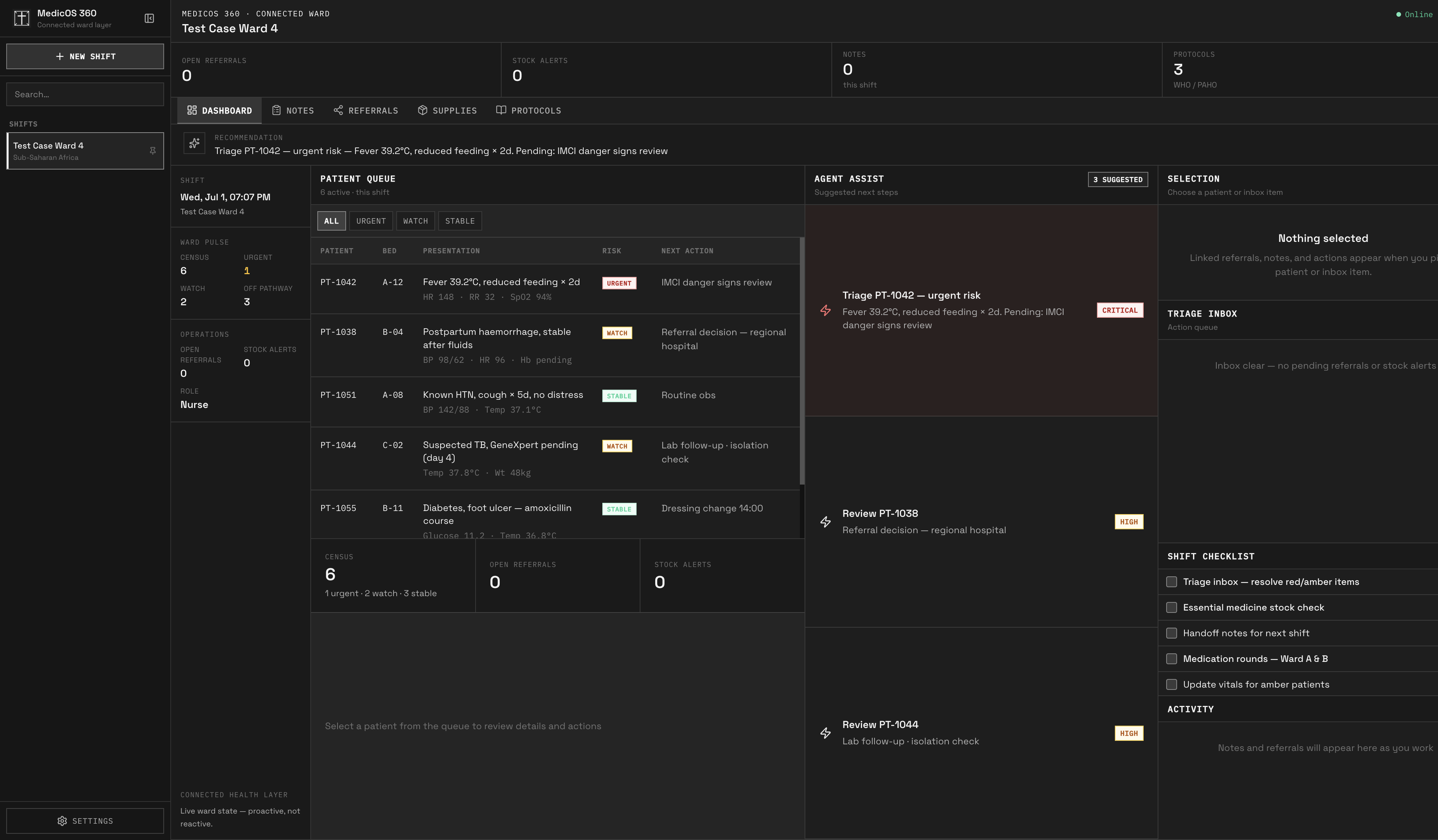
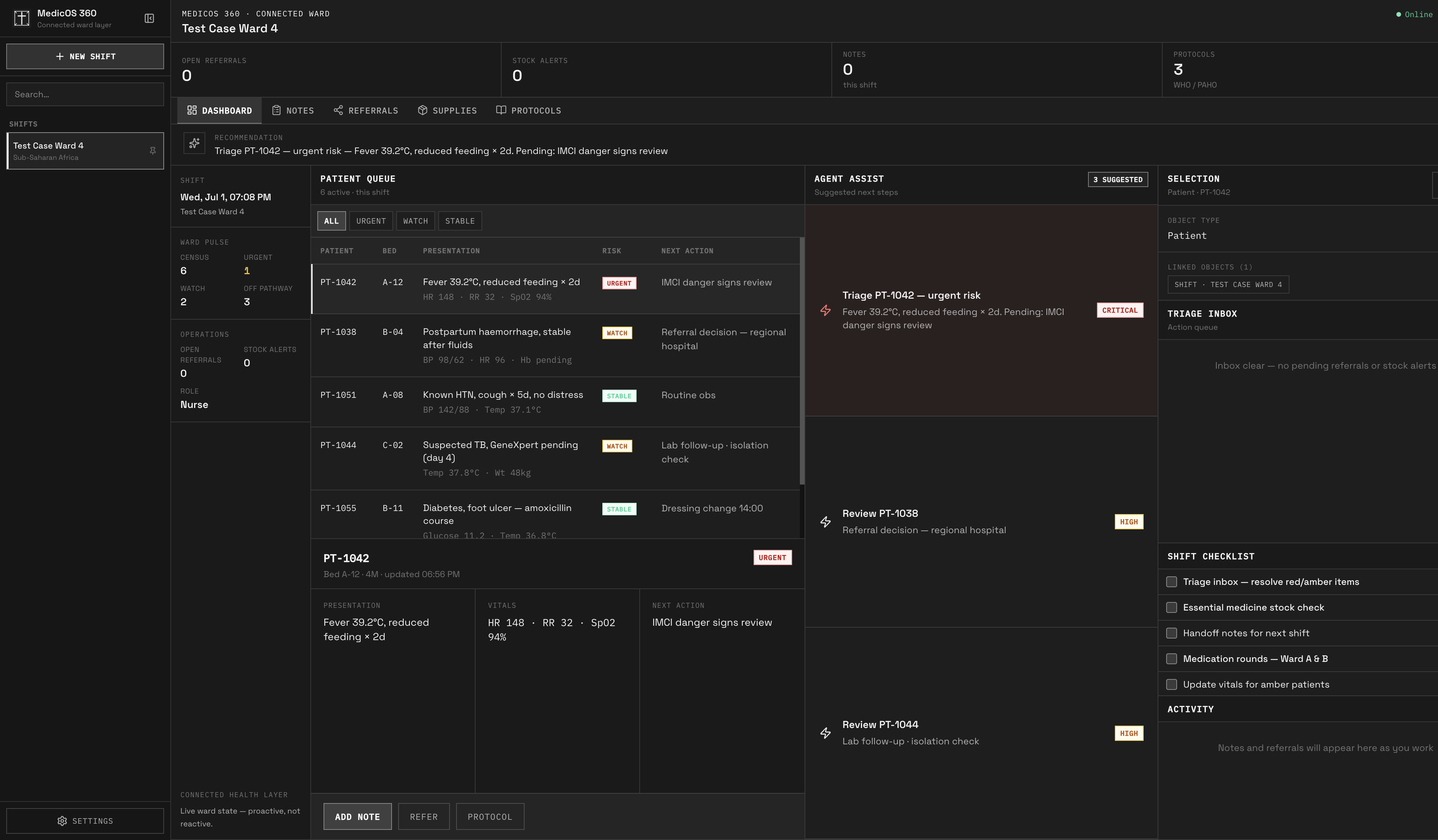
Fig 01 · Product surface
WardCanvas: ward truth in one canvas
Operational gaps
Six signals that break hospital throughput
| Signal | Observed in field | Operational impact | MedicOS response |
|---|---|---|---|
| Bed state opacity | Ward boards updated on whiteboards or WhatsApp; bed managers learn about discharges hours late. | ED boarding, cancelled surgeries, and informal payments to secure beds. | WardCanvas bed graph with expected discharge, isolation flags, and specialty constraints in one canvas. |
| Referral loop breakage | Referral slips, PDF attachments, and verbal handoffs with no closure signal back to the sending clinic. | Lost follow-up, duplicate labs, and patients who never arrive at the receiving service. | Referral rail with status, SLA timers, and receiving-service acknowledgment tied to the active encounter. |
| Protocol drift | Clinical pathways exist as binders or static PDFs; nurses improvise when stock or staffing changes mid-shift. | Antibiotic stewardship failures, missed sepsis bundles, inconsistent obstetric checklists. | Phase-aware protocol cards that bind to patient context, stock availability, and role permissions. |
| Supply fragmentation | Pharmacy, central store, and ward stock tracked in separate spreadsheets with manual reconciliation. | Stock-outs during surge weeks, expired batch usage, and emergency procurement at premium cost. | Unified supplies panel with lot traceability, reorder thresholds, and ward-level burn rate. |
| Notes without structure | Free-text notes in disconnected systems; night teams lack structured handoff summaries. | Repeated history taking, medication errors on shift change, weak medico-legal audit trails. | Structured notes with encounter linkage, template discipline, and export for ministry reporting windows. |
| No command view | Directors receive lagging PDF reports; charge nurses cannot see cross-ward pressure in real time. | Reactive staffing, missed outbreak signals, and capital plans disconnected from daily throughput. | WardCanvas command dashboard: occupancy, referral backlog, stock risk, and protocol variance in one surface. |
Regional profiles
Four contexts, one hospital operating problem
Hospital beds per 10,000 population (WHO GHO benchmarks)
Latin America
Brazil, Colombia, Peru, Haiti corridor
- EHR penetration
- 38%
- Referral delay
- 52h
- Stock-out index
- 64
- Beds / 10k
- 2.1
Lacking: Interoperability between public insurers, fragmented procurement, and specialist networks that span cities and rural clinics.
Africa
Kenya, Nigeria, Madagascar, Eritrea
- EHR penetration
- 22%
- Referral delay
- 78h
- Stock-out index
- 71
- Beds / 10k
- 1.3
Lacking: Shared device hygiene, offline sync discipline, CHW-to-hospital referral closure, and donor reporting that steals nurse time.
South Asia
Bangladesh, Nepal, Pakistan interior
- EHR penetration
- 19%
- Referral delay
- 65h
- Stock-out index
- 68
- Beds / 10k
- 0.9
Lacking: Bed management at scale, antibiotic tracking, and supervisor dashboards that work on low-bandwidth ward tablets.
Reference (OECD median)
Benchmark only
- EHR penetration
- 89%
- Referral delay
- 18h
- Stock-out index
- 12
- Beds / 10k
- 4.8
Lacking: Not applicable as operational target; useful as contrast for what default EHR products assume.

Operational reality: vitals, orders, and handoffs arrive faster than ward boards can reconcile. Supervisors need authoritative bed and patient state, not lagging summaries.

Supply blind spots remain the fastest path to preventable adverse events when formulary data lives outside the ward workflow.

Referral and triage queues collapse when intake, bed assignment, and specialist availability are not one continuous thread.
Platform
How MedicOS assists hospital operators
01
WardCanvas command canvas
A director-grade view of occupancy, referral pressure, stock risk, and protocol variance. Built for charge nurses and medical superintendents who need ward truth, not yesterday's PDF.
02
Referral continuity
Intake, routing, acknowledgment, and closure in one thread. Sending clinics see when patients arrive, when labs complete, and when the receiving service accepts responsibility.
03
Protocol execution
Pathways bind to patient context and role. Steps adapt when stock is unavailable or staffing changes, with variance captured for review instead of silent drift.
04
Supplies intelligence
Lot-level visibility from central store to ward cabinet. Burn rate, expiry risk, and reorder logic tuned for irregular delivery schedules common outside OECD supply chains.
05
Structured clinical notes
Encounter-linked documentation with handoff templates. Night teams inherit structured summaries instead of parsing unstructured paragraphs across systems.
06
Offline-aware sync
Ward capture continues when LAN drops. Conflict-safe sync when connectivity returns, with audit trails ministries and hospital boards can inspect.
Methods
Research questions
- RQ1
Which hospital signals must be visible at ward level versus director level without duplicating data entry?
- RQ2
How do referral SLAs differ across Latin American insurer networks, African county systems, and South Asian district hospitals?
- RQ3
What minimum ontology links patient, bed, referral, protocol step, stock lot, and note without forcing OECD-style ADT maturity?
- RQ4
Where can bounded automation reduce nurse clerical load while keeping physicians and supervisors on high-risk decision paths?
Baseline versus target endpoints for WardCanvas pilots
Stratir delivery
Forward-deployed hospital software
Stratir applies the same discipline used for intelligence and agentic products to hospital operations: ontology first, bounded automation, human review on high-risk paths, and exports partners can audit.
Discuss MedicOS research01
Ward ethnography
Stratir maps how beds are assigned, how referrals actually move, and where paper re-enters the workflow before any dashboard is designed.
02
Hospital ontology
Bed, encounter, referral, protocol, stock lot, and note entities modeled once so ward, pharmacy, and director views stay aligned.
03
WardCanvas build
Engineering ships command surfaces on shared ward hardware with role-based access, offline capture, and inspectable sync behavior.
04
Measured pilot
Pilots track referral closure, bed accuracy, stock-outs, and handoff compliance. Vanity logins are excluded from success criteria.
References
WHO Global Health Observatory
Hospital bed density, health workforce, and expenditure indicators by country.
World Bank WDI
Health expenditure, rural share, and connectivity proxies for regional comparison.
PAHO / Africa CDC frameworks
Regional reporting conventions for public hospital networks.
Stratir field observations
Site visits and design partner interviews across Latin America and Africa, 2024-2026.
MedicOS is a Stratir research program. Indicator values in charts are comparative framing anchored to published regional benchmarks and field observations. They must be validated against local ministry and hospital datasets before operational or procurement use. This brief is a systems research artifact, not clinical guidance.
Hospital deployments require explicit governance. Read Stratir Privacy and Civil Liberties for how we frame sensitive health data, operator access, and auditability in field programs.